

Photo credit to Barbara Olsen
Charlatans of our current time are rebranding an genre of snakeoil supplements and relaxation plans as revolutionary ways to improve health with minimal effort, or maximally misguided effort, depending on which guru is selling something. This "biohacking" movement is the latest in a long line of trendy ways to dupe the gullible into parting with their money by promising longevity or physical performance that is unrelated to the product being sold. While there is no doubt all of our health is the cumulative result of many personal decisions, luck in the genetic lottery, and luck with respect to avoiding accidents, the "biohacks" on offer tend to serve as a significant distraction more than anything. This article began as an exploration of the important actions within our control germane to longevity. It evolved into an exploration of testing protocols for VO2 max (This article is in the drafts folder for a reason: it lacks a coherent point).
There are no shortage of articles written by medical professionals and scientists who spend their careers analyzing epidemiological data. These articles [1,2,3,4] make clear that a person is likely to be healthiest and live longest if they: (1) are in the strongest 20% of the population [5,6,7], (2) have a VO2 max in the top 20% of the population (3) maintain a healthy body weight and body composition; BMI between 22 and 27 (4) sleep well and for sufficient periods of time daily [consistent timing, dark and cool environment] (5) avoid tobacco, alcohol, and other addictive intoxicants/poisons, (6) have a medical professional monitor a limited set of key parameters [cholesterol/ApoB, triglycerides, and blood pressure], (7) avoid using pharmacology to deal with pain, and (8) create meaningful social relationships.
This eight item list is easier said than done. Most people putting effort into their health will spend unjustifiable effort optimizing for one or two of these parameters. In general, your effort will provided the largest return on investment when concentrating on deficient areas rather than hyper optimizing a limited subset.
Since the 1980s, every school age child has been told how dangerous cigarettes are. However, they are virtually never told that cardiorespiratory fitness is more important. Moving from below average to above average in cardio fitness has the same effect on all cause mortality as moving from the smoking to non-smoking group. Moving from low fitness to elite fitness is 4 times as powerful as moving from the smoking to non-smoking group. [8] However, it is obviously difficult to be in the upper levels of cardiorespiratory fitness while smoking regularly. I am not arguing for smoking; I am arguing for fitness. Similarly, though to a less extreme degree, strength is highly important to longevity [9,10]. Some studies indicate it is more important than smoking, but this finding is not universally reproducible across studies.
Assessing physical strength is not particularly difficult. Any quantifiable resistance against a movement pattern produces a measurement more accurate than almost any measurement in medicine or sports physiology (up to four significant figures). This finding is subject to variability due to fatigue, blood sugar, arousal state, movement pattern familiarity, and effort. In normal situations this results in less than 10% variability. Grip strength is the most commonly reported metric but this is likely because it is highly correlated with total body strength and because it can be easily and relatively safely tested across a variety of demographics from the competitive strength athlete to the centurian in a nursing home.
VO2 max testing is another animal. Finding reliable testing protocols is still difficult. More on this below.
There is a U-shaped curve between BMI and all-cause mortality in large population studies [11,12]. Depending on the study, the BMI associated with longest lifespan is between 20 and 25. There is a lot of controversy around BMI because it is a coarse metric. A person's ideal body weight may not perfectly align with the standard BMI recommendations from population studies a number of reasons, though all such exceptions are uncommon. Most common is excess muscle mass. Someone with 10 to 40 kg of excess muscle from deliberate physical training will be healthier at their body weight than the same person with 10 to 40 kg of excess fat but BMI does not take this into account. Women with large mammary glands will have higher BMI's than otherwise equal women with smaller mammary glands but no study (that I know of) has shown large mammary glands to have a deleterious health effect. More uncommon still are anthropometric differences that change BMI without changing health outcomes. The neck and calf weight less per unit of height than the torso or thigh. The relative contribution of neck, calf, thigh, torso, and head to total body height is not constant across all humans. Therefore, a human with a long neck and long calves will have a lower ideal BMI than a person of the same height with a short neck and short calves.
What seems to be hard to understand for the general public intent on dismissing BMI as backwards out-of-date science is that BMI is a useful but incomplete metric. It is suitable for use as a guide toward a healthy body after correcting for exceptions that may apply to any specific case (excess muscle, breast tissue, or unusual anthropometric ratios). For all these protestations, it is rarely acknowledged that there is a better option. A DEXA scan, a test that costs under $200 will provide anyone who cares to know the gold standard level of information on their body composition. The DEXA scan does not need to be corrected based on dubious guesses about BMI exceptions, the DEXA will measure those exceptions for you. Whenever you are talking to someone who is intent on dismissing BMI, you can confidently assume they are more interested in ignoring their health than they are in learning about it if they have not had a DEXA scan recently.
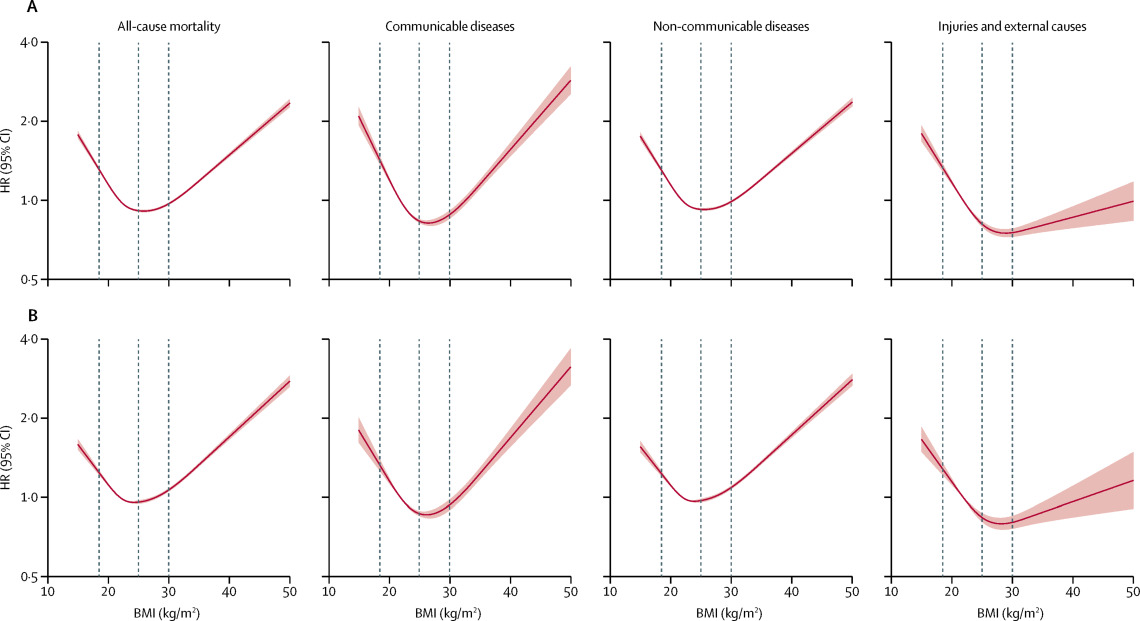
[Caption] Figure from [11].
Sleep [section to be completely later] is real important.
Recreational drugs [section to be completed later]. As a general rule, recreational drugs, legal or otherwise, are not good for you. In fine enough moderation, some drugs have a positive effect but it is rare that anyone making that argument is consuming small enough quantities for that argument to apply.
Having regular screening tests for cholesterol/triglycerides/ApoB (usually ordered a lipid panel), blood pressure, and a couple cancers (breast and prostate come to mind) definitely has a positive impact on your lifespan. Most cancer tests are not specific and sensitive enough to be valuable for the general population (ie the positive predictive value of most tests in low prevalence populations is uselessly low). If you have known risk factors for specific cancers, this may not be the case for you personally. However, everyone benefits from screening via lipid panels and blood pressure monitoring.
The last 20 years of the growing opioid epidemic has proven that regularly treating pain with pharmaceuticals does not work well for a significant fraction of the population. In 2022, 90,000 Americans died of opioid overdose compared to 3,500 in 1999. Over that same period, traffic fatalities killed 30,000 to 40,000 per year. For long term health, the best advice is to avoid modern medicine for pain management.
While social relationships are clearly important for long term healthspan and lifespan, the exact manner in which you can improve them is largely beyond the scope of this blog. There is little insight that engineering can give to improving social relationships.
Unfortunately towards the end of this section I discovered someone else had already written exactly the paper I was trying to write. You could read this section or you could read a better version by people who know the field well. They even have a better title [13].
respiratory exchange ratio (RER): RER is defined as the volumetric flow rate of CO2 out of the lungs divided by the volumetric flow rate of O2 into the lungs [14]. At rest this ratio is 0.5 to 0.8 in most people. During exercise, it is expected to peak around 1.1 to 1.3.
lactate: the conjugate base of lactic acid. Lactic acid has a pKa of 3.86 [15] while human blood has a pH near 7.4 [15]. Therefore the lactate anion is the dominant form of lactic acid in the blood stream. Lactate is the main cause of the burn associated with physical exertion.

[Caption] Structure of lactic acid from wikipedia.
During the preliminary research for this article, I noticed all of the important physiological measurements for quantifying long term health are measured regularly except the most predictive indicator (VO2 max). Strength is measured every time I go to the gym; drug use is obvious to at least the person using the drugs; blood pressure and weight are measured at nearly every doctor's appointment; and lipid panels are taken during annual physicals. Other parameters are difficult or impossible to measure: social relationships are impossible to rigorously quantify; sleep quality cannot be measured by a single number and doing a sleep study to properly quantify as much as possible about sleep patterns is a costly endeavor. The neglected measurement is VO2 max: it is a 30 minute test at most and it is more predicitive of longevity than any other factor. Out of curiousity as much as anything, I took two friends and went to a clinic to have VO2 max testing done. This is where the rabbit hole began.

[Caption] Results of VO2 max testing for 3 subjects. Subjects 1 and 2 are male, subject 3 is female. Subjects 1 and 3 weigh approximately 70 kg, subject 2 is approximately 90 kg. Subject 3 has testing anxiety so her heart rate is nearly independent of physical effort during the test. Testing was conducted with a variant of the Bruce protocol [16,17]: treadmill testing on an incline with speed increases every three minutes until failure.
VO2 testing and the concept of a plateau of oxygen consuption over time during heavy exertion was originally observed by Archibald Hill and Hartley Lupton in 1923 [18].
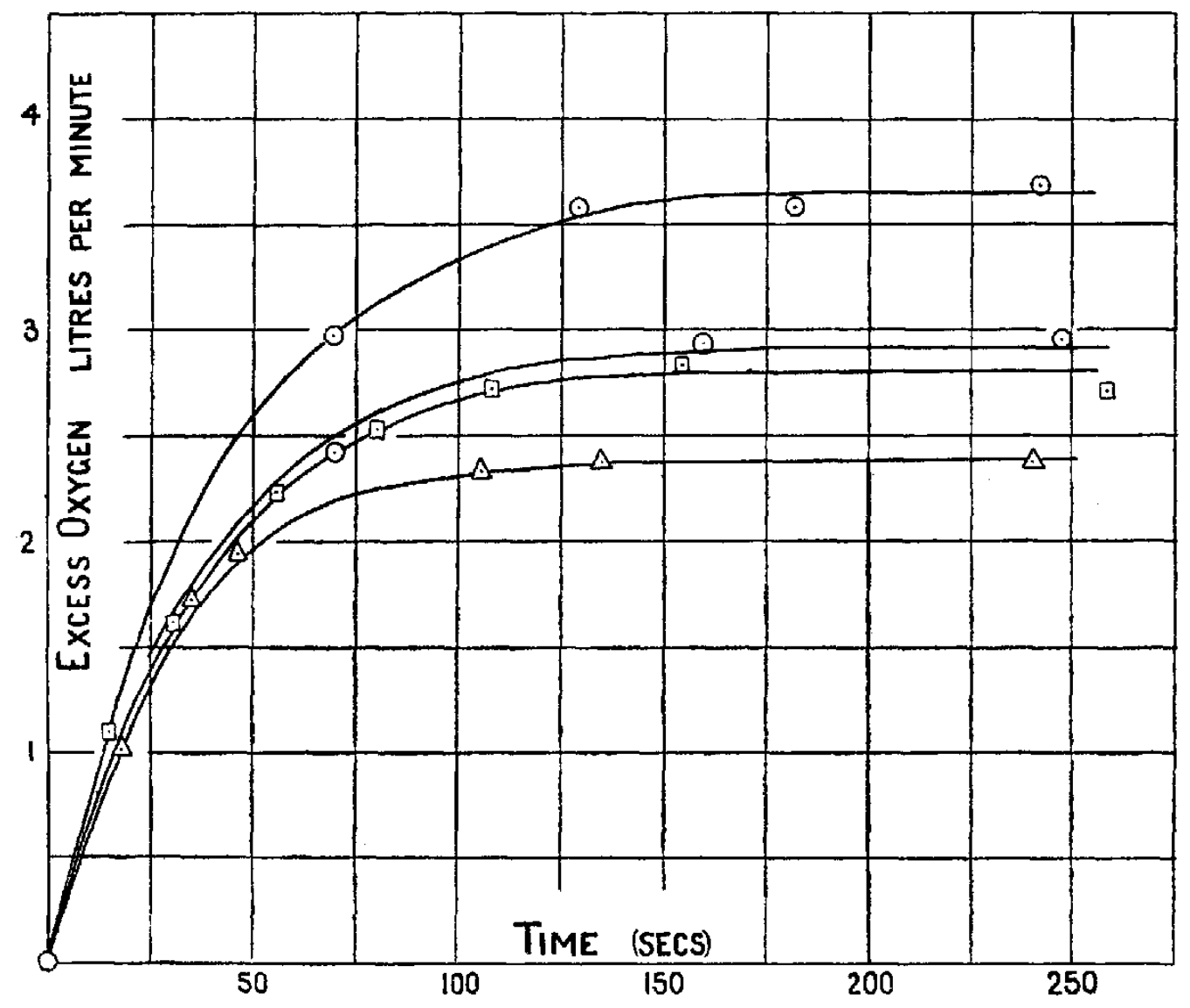
[Caption] Figure 2 from AV Hill 1923 [18]. First recording of a plateau in oxygen consumption vs time during exercise. This is the functional shape of the O2 vs time curve I was expecting but did not see in the VO2 testing I did with my friends. The lines in this graph are from a subject running at 3.0, 3.4, 3.4 (again), and 4.5 m/s.
The gold standard test is one where steady state O2 consumption is measured at a set of work rates and the O2 vs power function approaches an plateau. In healthy populations, this plateau is usually caused by reaching the limit of cardiac output [19]. If time and expense were not limiting factors, one could measure the steady state O2 consumption at a set of workrates with ample time for the subject to recover and measure a true VO2 max. This "true" test would have a procedure something like this: (1) Monitor the O2 consumption during exercise at a constant work rate until a plateau is reached measuring O2 consumption every 15 seconds. (2) Rest until the heart rate recovers to pre-test levels. (3) Repeat steps one and two for a series of work rates from trivial to unsustainable for greater than 120 seconds. The result would appear something like the sketch below (similar sketches appear in other sources [13,20]):

[Caption] Schematic of expected results from multistage VO2 max testing. NOT REAL MEASUREMENT DATA, fabricated for illustration purposes only.
In practice this is prohibitively expensive and not regularly done. Testing protocols from 1923-1963 were somewhat haphazard (do we measure O2 consumption vs time or vs exercise power output? constant or ramped work loads? etc, etc). In 1955, continuous testing was demonstrated to show a peak in oxygen uptake allowing VO2 max testing to be completed in a time efficient manner [21]. This is widely regarded as the seminal paper on oxygen uptake in continuous testing protocols. In 1963, Robert Arthur Bruce (1916-2004), chief of cardiology at the University of Washington Seattle and founder of Seattle Heart Watch [22], published a ramped exercise protocol which is still the basis of modern protocols for VO2 max testing today [17]. His incline treadmill test raised the speed and inclination every 3 minutes until the subject failed to continue. The exercise treadmill test (commonly abbreviated as ETT) was originally designed to assess cardiac patients. Today there are a lot of Bruce protocol variations which all claim to be more suitable for specific situations. A 2019 review attempted to list all of them [23] but the protocol used in my VO2 max test was not on their list of 14 "direct methods" (methods that require a gas analyzer instead of just making an estimate based on wattage and heart rate). The Ellestad Protocol is the closest to the protocol used in our test but even that involves changing the elevation at later stages (which was not the case where we were tested). All of the ETT protocols are some version of the following: 3 to 8 stages of work at a fixed treadmill speed and incline, increase the speed or incline at each stage with no breaks between stages.
There is still controversy today on the implementation of continuous testing protocols because such protocols do not reliably produce a plateau. Often, what is measured in the Bruce protocol (or its derivatives), is a VO2 peak (where no VO2 plateau is reached) not a true VO2 max. Some researchers think this is dodgy science and needs to be stopped [24], other researchers think that position is myopic [25]. The argument against continuous testing is that is does not reliably measure what is claimed. The argument for continuous testing is that it is the only affordable way to test large numbers of subjects. A Bruce protocol-style test can be run in under 20 minutes and often under 10. A "true" VO2 max test would take most of a day because the rest periods required on the higher wattage sub-tests would be longer than an entire Bruce protocol test.
If a test is terminated without a plateau, how do we decide when to end a test? The clearest criteria for calling a measurement a VO2 max comes from a book by the British Association of Sport and Exercise Sciences (BASS) [26]. Unfortunately this book seems to be out of print, but it is summarized in a number of places as defining the standards for VO2 max testing [27,28]. It specifies (i) subjective fatigue and volitional exhaustion (the tester should perceive the athlete to be exhausted), (ii) a plateau in the oxygen uptake/exercise intensity relationship (defined as an increase in oxygen uptake of less than 2 mL per kg per min or 5%), (iii) a final respiratory exchange ratio of 1.15 or above, (iv) heart rate within 10 bpm of age predicted max heart rate, and (v) the peak blood lactate concentration should be above 8 mmol per L. How many of these criteria or which combination must be met is unclear [27]. In practical application, studies that reference this set of standards typically say they conformed to the non-invasive standards of the BASS (i - iv) or just a subset of them [27,28,29]. Whatever the standard used, everyone seems to agree you should be very tired after a VO2 max test and they almost always agree you should observe a plateau in oxygen uptake. If you do not, then you measured a VO2 peak by terminating a test prematurely.
These standards are easily critized. First, since at least the 1970s, it has been documented that the heart rate achieved during a VO2 max test is highly variable [30] and max heart rate calulators are never recommend for determining the end point in exercise testing [31]. Second, there has been general disagreement for 40+ years on how to incorporate all the secondary criteria [32,33] and whether a verification day is required (a second test day at 105-120% of the work rate achieved on the previous incremental test showing the same VO2 max value) [34,35]. Third, as recently as 2020 there was some controversy about whether the VO2 max plateau was ever a real thing or if it was just a sampling and variability artifact [36,37,38]. That seems to have been settled in the direction of the plateau being a real physiological phenomenon [36].
A plateau in VO2 vs time or vs work is more commonly observed in subjects breathing lower O2 concentration air (15% or less O2 compared to 21% O2 in normal atmosphere) [39,40,41].
Equations to predict VO2 max based on age, weight, power output, and "leisure time score" are no more than +- 20% accurate or the "magnitude of the [error ... was] too large to be of practical value for estimating VO2 max" [42].
[1] "Where should my priorities be to improve my health?" Barbell Medicine Blog, 2020.
[2] "Eight Habits for Longevity: Life-Lengthening Factors Increase Lifespan by 24 Years," NeuroscienceNews.com, 2023.
[3] "Impact of healthy lifestyle factors on life expectancies in the US population," Circulation, vol. 138, pp. 345—355, 2018.
[4] "Healthy Longevity," The Nutrition Source, 2022.
[5] "Associations of muscle mass and strength with all-cause mortality among US older adults," Medicine and Science in Sports and Exercise, vol. 50, pp. 458, 2018.
[6] "Muscular strength as a predictor of all-cause mortality in an apparently healthy population: a systematic review and meta-analysis of data from approximately 2 million men and women," Archives of Physical Medicine and Rehabilitation, vol. 99, pp. 2100—2113, 2018.
[7] "Handgrip strength and all-cause mortality in middle-aged and older Koreans," International Journal of Environmental Research and Public Health, vol. 16, pp. 740, 2019.
[8] "Association of cardiorespiratory fitness with long-term mortality among adults undergoing exercise treadmill testing," JAMA Network Open, vol. 1, pp. e183605—e183605, 2018.
[9] "Midlife muscle strength and human longevity up to age 100 years: a 44-year prospective study among a decedent cohort," Age, vol. 34, pp. 563—570, 2012.
[10] "Independent and combined associations of upper and lower limb strength with all-cause mortality in community-based older adults: findings from the Chinese Longitudinal Healthy Longevity Survey," Public Health, vol. 220, pp. 57—64, 2023.
[11] "Association of BMI with overall and cause-specific mortality: a population-based cohort study of 3.6 million adults in the UK," The Lancet Diabetes & Endocrinology, vol. 6, pp. 944—953, 2018.
[12] "BMI and all cause mortality: systematic review and non-linear dose-response meta-analysis of 230 cohort studies with 3.74 million deaths among 30.3 million participants," British Medical Journal, vol. 353, 2016.
[13] "The oxygen uptake plateau — A critical review of the frequently misunderstood phenomenon," Sports Medicine, vol. 51, pp. 1815—1834, 2021.
[14] "Predicting postoperative complications with the respiratory exchange ratio after high-risk noncardiac surgery: a prospective cohort study," European Journal of Anaesthesiology, vol. 37, pp. 1050—1057, 2020.
[15] "Chapter 2 - Water: The medium of life," in Biochemistry 6ed, pp. 42—46, 2016.
[16] "Exercising testing in adult normal subjects and cardiac patients," Pediatrics, vol. 32, pp. 742—756, 1963.
[17] "On the 50th anniversary of the first description of a multistage exercise treadmill test: re-visiting the birth of the Bruce protocol," Heart, vol. 99, pp. 1793—1794, 2013.
[18] "Muscular exercise, lactic acid, and the supply and utilization of oxygen," QJM: Quarterly Journal of Medicine, pp. 135—171, 1923.
[19] "Health-related physical fitness testing and interpretation," in Guidelines for exercise testing and prescription, eighth edition, pp. 60-102, 2010.
[20] "The peak versus maximum oxygen uptake issue," CPX International, pp. 1—9, 2010.
[21] "Maximal oxygen intake as an objective measure of cardio-respiratory performance," Journal of Applied Physiology, vol. 8, pp. 73—80, 1955.
[22] "Seattle Heart Watch: initial clinical, circulatory and electrocardiographic responses to maximal exercise," The American Journal of Cardiology, vol. 33, pp. 459—469, 1974.
[23] "A review: Maximal oxygen uptake (VO2 max) and its estimation methods," Internation Journal of Physical Education, Sports, and Health, vol. 6, pp. 24—32, 2019.
[24] "Measurement of the maximum oxygen uptake Vo2max: Vo2peak is no longer acceptable," Journal of Applied Physiology, vol. 122, pp. 997—1002, 2017.
[25] "VO2peak is an acceptable estimate of cardiorespiratory fitness but not VO2max," Journal of Applied Physiology, vol. 125, pp. 229—232, 2018.
[26] Guidelines for the physiological testing of athletes, 1997.
[27] "Measurement of maximal oxygen uptake from two different laboratory protocols in runners and squash players," Medicine and Science in Sports and Exercise, vol. 31, pp. 1226—1229, 1999.
[28] "The repeatability and criterion related validity of the 20 m multistage fitness test as a predictor of maximal oxygen uptake in active young men," British Journal of Sports Medicine, vol. 39, pp. e19—e19, 2005.
[29] "Endurance running performance after 48 h of restricted fluid and/or energy intake," Medicine and Science in Sports and Exercise, vol. 39, pp. 316, 2007.
[30] "Criteria for maximum oxygen uptake in men over 40 in a population survey," Medicine and Science in Sports, vol. 4, pp. 18—22, 1972.
[31] Guidelines for exercise testing and prescription, 1991.
[32] "Tests of maximum oxygen intake a critical review," Sports Medicine, vol. 1, pp. 99—124, 1984.
[33] "Criteria for maximal oxygen uptake: review and commentary," Medicine & Science in Sports & Exercise, vol. 27, pp. 1292—1301, 1995.
[34] "How to test maximal oxygen uptake: a study on timing and testing procedure of a supramaximal verification test," Applied Physiology, Nutrition, and Metabolism, vol. 36, pp. 153—160, 2011.
[35] "The maximal oxygen uptake verification phase: a light at the end of the tunnel?" Sports Medicine-open, vol. 3, pp. 1—15, 2017.
[36] "Oxygen uptake plateau: calculation artifact or physiological reality?" European Journal of Applied Physiology, vol. 120, pp. 231—242, 2020.
[37] "High prevalence of false-positive plateau phenomena during VO2max testing in adolescents," Journal of Science and Medicine in Sport, vol. 17, pp. 526—530, 2014.
[38] "Effect of sampling on variability and plateau in oxygen uptake," Journal of Applied Physiology, vol. 68, pp. 404—410, 1990.
[39] "Incidence of the oxygen plateau at VO2max during exercise testing to volitional fatigue," Journal of Exercise Physiology Online, vol. 3, pp. 1—12, 2000.
[40] "Effects of FO2 on leg VO2 during cycle ergometry in sedentary subjects," Medicine and Science in Sports and Exercise, vol. 30, pp. 697—703, 1998.
[41] "Effects of oxygen fraction in inspired air on rowing performance.," Medicine and Science in Sports and Exercise, vol. 27, pp. 573—579, 1995.
[42] "Validity of VO2max equations for aerobically trained males and females," Medicine & Science in Sports & Exercise, vol. 36, pp. 1427—1432, 2004.